
Sometimes the equipment is the easy part. The harder part is everything around it.
Who gives the medications on schedule? Who monitors the wound site? Who helps your parent to the bathroom at 3am? Who notices when something isn’t right — a low-grade fever, increasing confusion, a leg that’s more swollen than yesterday? The domestic help can’t do this. Your mother, who may be elderly herself, shouldn’t have to.
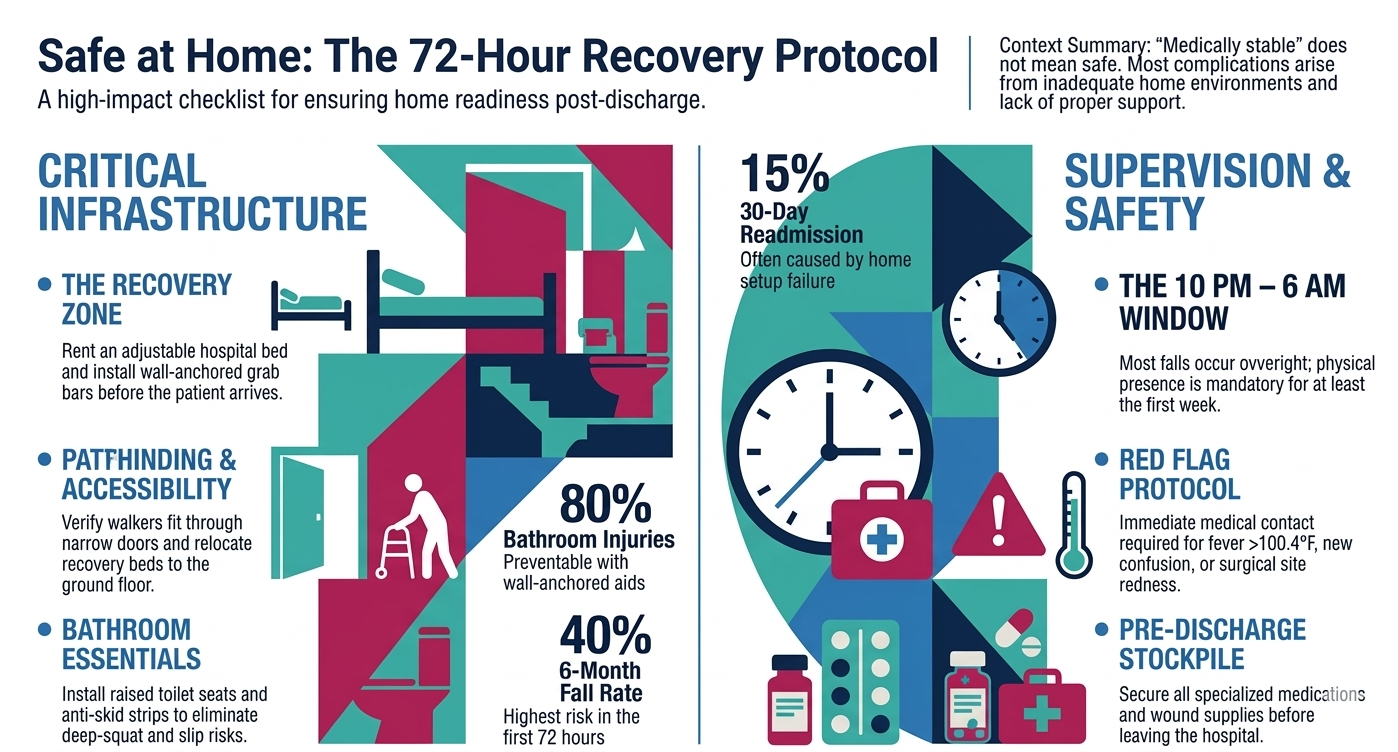
This is where care for elderly parents shifts from a logistics problem to a supervision problem. Post hospital care for an elderly parent isn’t just about having the right bed and the right grab bar. It’s about having someone trained and present — especially in the first two weeks — who knows what to watch for and when to escalate. Research shows that up to 40% of elderly patients fall within 6 months of hospital discharge, and the highest risk is concentrated in the first few weeks when the patient is weakest and the home is least prepared.
For NRI families, this is often the moment of truth. You can’t fly back for every discharge. You shouldn’t have to. But the gap between what your mother says is fine and what’s actually happening in that flat is where things go wrong. Having a professional on the ground — someone who reports to you, not just to your parents — changes the equation entirely.
